
Ambulatory Blood Pressure Monitor: A Complete Clinical Guide
Hypertension remains one of the leading modifiable risk factors for cardiovascular disease worldwide. Yet for all the progress medicine has made in understanding and treating it, the basic act of measuring blood pressure in a clinical setting is still deeply imperfect. That is where the Ambulatory Blood Pressure Monitor steps in — offering a more complete, more honest picture of a patient’s true hemodynamic state than any single office reading ever could.
This guide covers how ambulatory monitoring works, why it matters clinically, what to look for in a device, and how it fits into modern hypertension management.
What Is an Ambulatory Blood Pressure Monitor?

An ambulatory blood pressure monitor is a portable, wearable device that automatically measures and records a patient’s blood pressure at regular intervals over a 24-hour period — or sometimes longer. Unlike a standard office sphygmomanometer, it captures readings while the patient goes about their daily life: working, eating, sleeping, commuting.
Readings are typically taken every 20–30 minutes during waking hours and every 30–60 minutes during sleep, producing a dataset of 50 or more measurements. This dataset is then analysed to extract a range of clinically meaningful parameters, including mean daytime and nighttime blood pressure, nocturnal dipping ratio, morning surge, and blood pressure load.
Why Office Readings Alone Are Not Enough
The limitations of office-based blood pressure measurement have been recognised for decades. Research consistently shows that a single reading taken in a clinic can overestimate a patient’s true blood pressure in 15–30% of cases. This is partly due to the well-documented white coat effect — an anxiety-driven elevation that occurs specifically in clinical environments.
Beyond white coat hypertension, there are other patterns that office readings simply cannot reveal:
Masked hypertension: Normal readings in the clinic but elevated readings in daily life. Affects an estimated 10–15% of the population and carries significant cardiovascular risk.
Nocturnal non-dipping: Blood pressure should naturally drop by 10–20% during sleep. Patients who fail to show this pattern — non-dippers — face substantially higher rates of stroke and organ damage.
Morning surge: A sharp rise in blood pressure in the hours after waking, associated with increased risk of cardiovascular events in the early morning hours.
None of these phenomena are detectable from a clinic visit. Ambulatory monitoring is the only reliable way to identify them.
Clinical Guidelines Supporting Ambulatory Monitoring
The evidence base for ambulatory blood pressure monitoring is extensive, and it is reflected in major clinical guidelines:
NICE (UK, 2019): Recommends ABPM as the method of choice for confirming hypertension in adults with elevated clinic readings.
2018 ESC/ESH Guidelines: Strongly recommend out-of-office measurement — including ABPM — for detecting white coat and masked hypertension, and for assessing treatment efficacy.
American Heart Association: Recognises ABPM as an important tool for diagnosing hypertension and evaluating antihypertensive treatment.
These are not fringe recommendations. Ambulatory monitoring has moved to the centre of evidence-based hypertension management.
Key Features to Evaluate in an ABPM Device

Not all ambulatory monitors are created equal. When selecting a device for clinical use, the following criteria deserve careful consideration:
Clinical Validation
The device should be validated against an established protocol such as the British Hypertension Society (BHS) standard or the AAMI/ANSI SP10 protocol. Manufacturers unwilling to provide validation documentation should be viewed with caution.
Patient Comfort
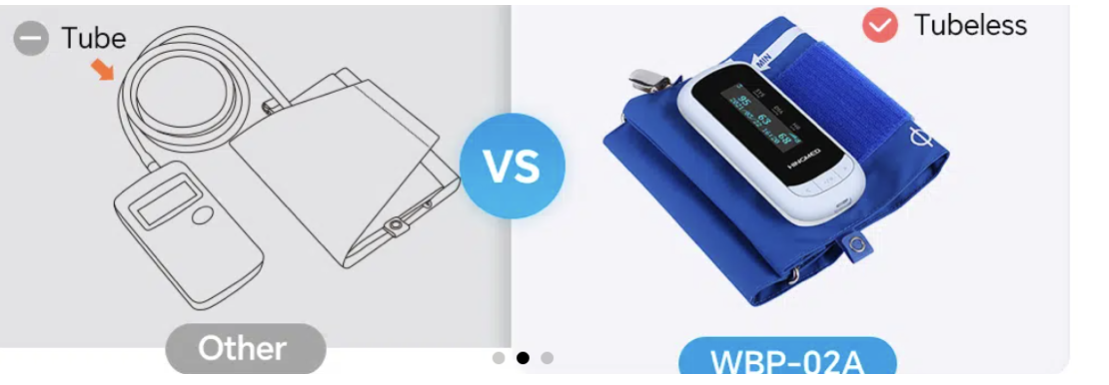
A monitor that disrupts sleep produces poor nocturnal data. The most significant design variable in this regard is whether the device separates the recorder unit from the cuff via rubber tubing, or integrates both into a single wearable unit. Newer all-in-one designs from manufacturers like
Newer all-in-one designs from manufacturers like hingmed — such as the WBP-02A, which combines the recorder and cuff in a single tubeless unit — substantially reduce sleep disruption and improve the quality of overnight readings.
Data Analysis Software
The clinical value of ambulatory monitoring depends on the quality of the analysis it produces. Look for software that generates structured reports covering mean values by time period, dipping classification, blood pressure load, and morning surge measurements. Integration with standard EMR formats is a practical necessity for most hospital settings.
Motion Artifact Handling
Readings taken during patient movement are prone to artifact. Robust motion-filtering algorithms reduce the number of rejected readings and improve the accuracy of the final dataset, particularly for active patients.
How Ambulatory Monitoring Improves Clinical Outcomes
The practical benefits of integrating ABPM into routine hypertension management are well documented. Several large-scale prospective studies have shown that cardiovascular outcomes correlate more strongly with ambulatory blood pressure values than with office readings. The most notable of these is the Syst-Eur trial and the PAMELA study, both of which demonstrated that 24-hour mean blood pressure is a superior predictor of left ventricular hypertrophy and overall cardiovascular risk.
For antihypertensive treatment, ambulatory monitoring provides a uniquely valuable window into whether a drug is actually working across the full dosing interval. A beta-blocker that controls office readings may still leave a patient’s early morning blood pressure inadequately managed. ABPM reveals this; a clinic visit does not.
Common Questions About ABPM
Is ambulatory monitoring uncomfortable for patients?
Most patients adapt to wearing an ABPM device within the first few hours. Discomfort is primarily related to the inflation of the cuff during measurement, which is brief. Sleep disruption varies by device design; tubeless, all-in-one monitors tend to be better tolerated overnight than traditional dual-unit designs.
How many readings are needed for a valid result?
Most validation protocols require at least 14 daytime readings and 7 nighttime readings for a monitoring session to be considered clinically valid. Modern devices flag when minimum thresholds are not met, allowing clinicians to decide whether a repeat session is warranted.
Can ABPM be used to monitor treatment response?
Yes, and this is one of its most valuable applications. Serial ABPM sessions before and after medication adjustment provide objective, time-resolved evidence of treatment efficacy across the full dosing period.
Conclusion
The Ambulatory Blood Pressure Monitor represents a genuine diagnostic advance — one that is now firmly embedded in clinical guidelines and standard hypertension care. It is not a replacement for clinical judgment, but it provides the kind of comprehensive, real-world data that clinical judgment requires. As device design continues to improve and patient tolerance increases, widespread adoption is not just clinically justified. It is increasingly necessary for responsible hypertension management.